
What if feeling short of breath isn’t always a lung problem?
Shortness of breath, or dyspnea (the uneasy sense you can’t get enough air), has many causes.
It can come on suddenly or creep up over weeks.
Some causes are simple, like being out of shape or anxiety.
Others are urgent, like a blood clot in the lung, heart failure, or a severe allergic reaction.
This post lays out the main causes, the warning signs to never ignore, and the simple things to track so you know what to do next.
Key Medical Reasons Behind Difficulty Breathing (Immediate Answers to What Causes It)

Breathing normally means your respiratory system pulls oxygen in and pushes carbon dioxide out at a steady rhythm, about 12 to 20 breaths each minute, without you having to think about it. Your oxygen saturation, which measures how much oxygen is in your blood, should sit between 95 and 100 percent. When breathing feels hard, labored, or like you can’t get enough air, that sensation is called dyspnea. Something is interfering with that automatic process.
Difficulty breathing can start suddenly or creep up slowly over weeks. The cause might be as simple as being out of shape or as serious as a blocked artery in the lungs. The pattern matters. Did it hit you out of nowhere, or has it been building for months? Are you wheezing, coughing, or feeling chest tightness along with it? Those clues help narrow down what’s going on.
Most cases fall into a few broad categories. Some involve the airways or lungs themselves. Others trace back to the heart or blood vessels. A few are tied to anxiety, blood problems, or severe allergic reactions. Here’s a quick look at the core groups:
Airway and lung conditions like asthma, COPD, pneumonia, or bronchitis
Heart problems including heart failure, arrhythmias, or reduced blood flow to the heart
Blood clots or circulation issues such as pulmonary embolism
Severe allergic reactions (anaphylaxis) that cause airway swelling
Blood disorders like anemia that reduce oxygen carrying capacity
Panic or anxiety that trigger rapid, shallow breathing even when the lungs and heart are fine
Respiratory Causes of Difficulty Breathing (Airway and Lung-Related Factors)

When the airways or lungs are inflamed, blocked, or infected, every breath takes extra effort. These respiratory causes are among the most common reasons people feel short of breath.
Asthma
Asthma narrows the airways in episodes. The muscles around the airways tighten, the lining swells, and extra mucus builds up. You might hear wheezing, a high pitched whistle when you breathe out. Chest tightness is common. Breathing can go from normal to difficult in minutes. Triggers vary: pollen, pet dander, cold air, exercise, or strong smells. If you use a rescue inhaler and symptoms ease within 15 or 20 minutes, that points to asthma. If the inhaler doesn’t help, or if breathing keeps getting worse, you need urgent care. Asthma can be mild and occasional, or it can flare into a serious attack that needs emergency treatment.
COPD
Chronic obstructive pulmonary disease is permanent damage to the lungs, usually from years of smoking. It includes chronic bronchitis, where the airways stay inflamed and produce thick mucus, and emphysema, where the tiny air sacs in the lungs break down. The hallmark is progressive breathlessness, especially during activity like climbing stairs or walking uphill. You might have a chronic cough that won’t quit. COPD builds slowly, often showing up after age 40 in people with a smoking history. It doesn’t go away. But quitting smoking slows the damage and helps you breathe easier over time.
Lung Infections
Pneumonia and bronchitis are infections that inflame the airways or fill parts of the lungs with fluid or pus. Pneumonia often brings fever, a cough that produces thick or colored mucus, and sharp chest pain that gets worse when you breathe deeply or cough. Bronchitis causes a persistent cough, chest discomfort, and sometimes wheezing. COVID-19 can also cause difficulty breathing, ranging from mild to severe. A chest X-ray usually shows abnormal spots or cloudiness if pneumonia is present. Bacterial pneumonia needs antibiotics. Viral infections like COVID-19 may need supportive care, monitoring, and sometimes oxygen therapy.
Serious or Life-Threatening Causes of Difficulty Breathing (Urgent Warning Signs)

Some causes of dyspnea are medical emergencies that require immediate action. These conditions can worsen rapidly and may be life threatening without quick treatment.
Pulmonary embolism happens when a blood clot, often from a leg vein, travels to the lungs and blocks blood flow. The onset is sudden. You might feel sharp chest pain that gets worse when you breathe in, cough up blood, or notice swelling in one leg. Oxygen levels can drop fast. Diagnosis usually requires a CT pulmonary angiography scan, and treatment involves blood thinners or clot dissolving drugs.
Anaphylaxis is a severe allergic reaction that can close off your airway within minutes. Common triggers include nuts, shellfish, bee stings, or certain medications. Along with difficulty breathing, you may develop hives, facial or throat swelling, stomach pain, or dizziness. If you have an epinephrine auto-injector, use it right away and call emergency services. Waiting can be fatal.
Pneumothorax, or collapsed lung, occurs when air leaks into the space between the lung and chest wall. You’ll usually feel sudden, sharp pain on one side of the chest along with breathlessness. It can happen spontaneously, especially in tall, thin young adults, or after chest trauma. A large pneumothorax may need a chest tube to reinflate the lung.
| Condition | Hallmark Sign |
|---|---|
| Pulmonary Embolism | Sudden breathlessness, sharp chest pain, possible blood in cough, leg swelling |
| Anaphylaxis | Rapid onset after allergen exposure, throat tightness, swelling, hives, collapse |
| Pneumothorax | Sudden one-sided sharp chest pain, breathlessness, may worsen quickly |
Heart-Related Causes of Difficulty Breathing (Cardiac Contributions)
The heart and lungs work closely together. When the heart can’t pump blood effectively, fluid can back up into the lungs, making it harder to breathe.
Heart failure means the heart muscle is too weak or stiff to move blood efficiently. Fluid accumulates in the lungs, especially when you lie flat. That’s why people with heart failure often prop themselves up with pillows at night or wake up gasping for air. This pattern is called orthopnea (breathlessness when lying down) or paroxysmal nocturnal dyspnea (sudden nighttime breathlessness). Swelling in the legs and feet is common. Heart failure develops over time, often from high blood pressure, prior heart attacks, or heart valve problems. It requires ongoing medication and regular follow up.
Arrhythmias are irregular or too fast heartbeats. Atrial fibrillation causes a chaotic, irregular rhythm. Supraventricular tachycardia is a regular but rapid heartbeat. Both can reduce the heart’s ability to pump blood, leaving you short of breath, dizzy, or weak. These conditions usually need medical evaluation and treatment to control the rhythm.
Angina and reduced coronary blood flow happen when the arteries supplying the heart muscle narrow. You might feel chest tightness or pressure, especially during exertion, along with breathlessness. This is a warning sign of coronary artery disease and should be evaluated promptly.
Anxiety, Panic, and Stress-Related Difficulty Breathing (Non-Physical Causes)

Not all difficulty breathing stems from a physical problem in the lungs or heart. Anxiety and panic attacks can trigger hyperventilation, rapid shallow breathing that makes you feel like you can’t get enough air.
During a panic attack, your body’s fight or flight response kicks in. Your heart races, you might feel chest tightness, and breathing speeds up. The episode usually peaks within minutes and then fades. You might also feel dizzy, tingly, or intensely afraid. If you’re certain it’s a panic attack and not a medical emergency, slowing your breathing or using grounding techniques can help.
Common panic attack symptoms include:
Rapid, shallow breathing or feeling like you can’t catch your breath
Chest tightness or discomfort
Heart palpitations or a racing heartbeat
Dizziness, tingling in hands or face, or a sense of unreality
If you’re not sure whether it’s anxiety or something else, especially if it’s your first time experiencing these symptoms, get checked out. Better safe than sorry.
Symptom Patterns That Help Identify the Cause of Difficulty Breathing
The timing and setting of your symptoms offer important clues about the underlying cause.
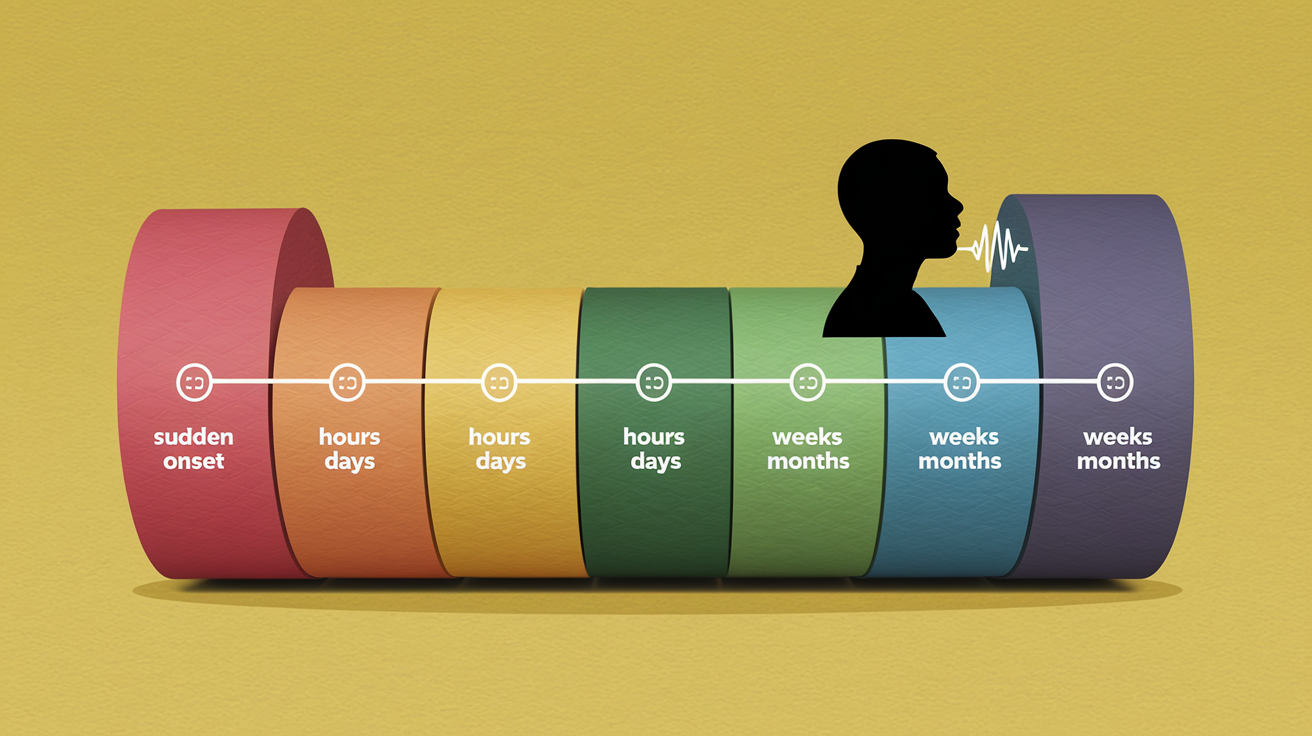
Sudden onset, happening in seconds to minutes, points to serious conditions like pulmonary embolism, pneumothorax, anaphylaxis, or a foreign object blocking the airway. If breathlessness develops over hours to a day or two, think asthma flare, pneumonia, or acute heart failure. Gradual worsening over weeks to months suggests chronic conditions like COPD, uncontrolled heart failure, or severe anemia.
Pay attention to these patterns:
Sudden (seconds to minutes): pulmonary embolism, pneumothorax, anaphylaxis, choking
Hours to days: asthma exacerbation, pneumonia, acute pulmonary edema
Weeks to months: COPD progression, chronic heart failure, interstitial lung disease
Worse when lying flat: heart failure (orthopnea)
Worse with activity, better at rest: deconditioning, obesity, early heart or lung disease
Associated with fever or cough: lung infection, bronchitis
What Doctors Check When Evaluating Difficulty Breathing (Diagnostic Process)

When you report difficulty breathing, clinicians start with a focused history and physical exam, then move to tests that measure how well your lungs and heart are working.
Pulse oximetry is a simple, noninvasive test. A small device clips onto your fingertip and measures oxygen saturation. Normal is 95 to 100 percent. Below 94 percent is concerning. Below 90 percent is an emergency threshold, often prompting oxygen therapy or urgent imaging. Respiratory rate is counted during the exam. Normal is 12 to 20 breaths per minute. A rate over 20 is tachypnea. Over 30 is severe and suggests respiratory distress.
Imaging and lab tests follow. A chest X-ray can reveal pneumonia, a collapsed lung, or an enlarged heart. An ECG (electrocardiogram) checks for heart rhythm problems or signs of reduced blood flow to the heart. Blood tests like a complete blood count (CBC) can identify anemia or infection. A BNP (B-type natriuretic peptide) test helps diagnose heart failure. If a pulmonary embolism is suspected, a D-dimer blood test and CT pulmonary angiography may be ordered.
| Test | What It Reveals |
|---|---|
| Pulse Oximetry | Oxygen saturation; normal 95–100%, concerning <94%, emergency <90% |
| Chest X-ray | Pneumonia, pneumothorax, heart size, fluid in lungs |
| CBC (Complete Blood Count) | Anemia, infection, elevated white blood cells |
| ECG (Electrocardiogram) | Heart rhythm abnormalities, signs of heart attack or strain |
Treatments for Difficulty Breathing Based on the Cause

Treatment depends entirely on what’s causing the breathlessness. There’s no one size fits all fix.
For asthma, a short acting bronchodilator inhaler (like albuterol) opens the airways quickly. If symptoms don’t improve within 15 to 20 minutes, or if they worsen, seek emergency care. Severe asthma attacks may need oral or IV corticosteroids to reduce inflammation. COPD is managed with long acting bronchodilators and inhaled steroids, plus smoking cessation. Pneumonia caused by bacteria requires antibiotics. Viral pneumonia or COVID-19 may need supportive care, oxygen, and monitoring. Pulmonary embolism is treated with anticoagulants (blood thinners) and sometimes clot dissolving drugs. Anaphylaxis demands immediate epinephrine, usually from an auto-injector, followed by emergency medical care.
Common treatment approaches include:
Bronchodilators for asthma and COPD to open airways
Oxygen therapy to raise oxygen levels when they drop too low
Antibiotics for bacterial lung infections like pneumonia
Anticoagulation (blood thinners) for pulmonary embolism
Epinephrine for severe allergic reactions
Chronic conditions like heart failure require diuretics to remove excess fluid, along with medications that support heart function. Severe anemia may be treated with iron supplements or, in urgent cases, blood transfusion.
When to Seek Medical Help for Difficulty Breathing (Urgency Levels)

Knowing when to call for help can save your life or someone else’s.
Get emergency care immediately if you experience sudden, severe breathlessness, especially if it comes with chest pain or pressure. Blue lips or fingertips (cyanosis) are a red flag. So is being unable to speak in full sentences because you can’t catch your breath. If your oxygen saturation drops below 90 percent, or if your breathing rate climbs above 30 breaths per minute, don’t wait.
Call 911 or go to the emergency department if you notice:
Sudden, severe difficulty breathing or gasping for air
Chest pain or tightness along with breathlessness
Blue or gray lips, face, or fingertips
Confusion, fainting, or loss of consciousness
For less urgent but still concerning symptoms like mild breathlessness with a known chronic condition, contact your primary care provider or visit urgent care within 24 to 72 hours. Persistent or worsening symptoms deserve evaluation even if they’re not dramatic.
Long-Term Prevention and Risk Reduction for Breathing Problems

Many causes of difficulty breathing can be prevented or managed with consistent lifestyle changes and medical follow up.
Smoking is the single biggest modifiable risk factor for chronic lung disease. Quitting reduces inflammation, slows COPD progression, and lowers the risk of lung infections and asthma flare ups. Vaccinations help, too. Annual flu shots and pneumococcal vaccines reduce the chance of severe respiratory infections that can trigger breathing crises.
Weight management and regular exercise strengthen the cardiovascular and respiratory systems. Even modest weight loss can ease breathlessness in people with obesity. Regular aerobic activity improves lung capacity and heart efficiency. If you have asthma or COPD, work with your clinician to create an action plan. Know your triggers, use controller medications as prescribed, and keep a rescue inhaler on hand. Environmental control matters. Avoid secondhand smoke, reduce exposure to allergens and air pollution, and manage indoor air quality. These steps won’t eliminate every risk, but they do lower the odds of serious breathing problems down the road.
Final Words
We started with quick answers: normal breathing ranges, what “difficulty breathing” means, and the main medical categories behind it.
Next we looked at lung-related causes like asthma and infections, heart-related issues, anxiety and panic, urgent red flags, tests, and treatments.
Keep a simple log of when it started, what makes it better or worse, how long episodes last, and oxygen or breathing rate changes.
If you use these steps to track symptoms and ask the right questions, you’ll be clearer about possible causes of difficulty breathing and ready to get the care you need.
FAQ
Q: Why do I feel like I can’t take a full breath or like I’m not getting enough oxygen?
A: Feeling like you can’t take a full breath or like you’re not getting enough oxygen usually reflects shallow or restricted breathing. Common causes are anxiety, asthma, lung infection, or anemia. Get urgent care for chest pain or blue lips.
Q: What is the most common cause of difficulty breathing?
A: The most common cause of difficulty breathing is airway or lung problems such as asthma and allergies; anxiety and deconditioning are also frequent, while infections or heart issues vary by age and history.
Q: How do I tell if my shortness of breath is serious?
A: You can tell shortness of breath is serious if it starts suddenly, stops you speaking in full sentences, causes chest pain, fainting, blue lips, very fast breathing, or oxygen saturation below 94%.